In this NIHR Invention for Innovation (i4i) project we developed an endoscopic optical coherence tomography (OCT) system for laryngeal imaging and performed trials at Northwick Park Hospital.
Laryngeal cancer (cancer of the larynx or voicebox) is one of the most common primary head and neck cancers, with smoking and alcohol as the main risk factors. Treatment of early-stage laryngeal cancer by laser ablation through the mouth has a cure rate of over 90%, avoiding the side effects of radio/chemotherapy and providing better functional recovery for vocal and swallowing functions. Conversely, later stage laryngeal cancer is hugely expensive to treat and wasteful of healthcare resources, often requiring mutilating treatment which results in the loss of ability to speak and/or swallow. Early diagnosis and treatment is therefore critical.
This project investigated the use of Optical Coherence Tomography (OCT), a relatively new tissue imaging modality, for early diagnosis of laryngeal cancer. A complex light probe was developed and used for scanning the tissue’s surface, penetrating up to a few millimeters deep, and obtaining accurate information regarding the tissue characteristics. Without the need to physically cut into tissue in order to examine its microstructure to determine if it is normal, pre-cancerous or cancerous, this method allows for non-invasive “optical biopsy”. In vivo and ex vivo studies have shown that high-resolution OCT images correlate well with histology sections for normal tissue, with the ability to distinguish healthy from unhealthy tissue in various organs.
This project was a pilot / feasibility study building on prior basic research, applying an existing and rapidly evolving technology (used successfully in ophthalmology) to address an urgent healthcare need; that of diagnostic cancer screening for which there is a strong clinical pull from within the UK National Health Service (NHS).
The first phase of the project involved ex vivo study of laryngeal tissue taken from laryngectomy patients at the host clinical site, Northwick Park Hospital in London. These were prepared and mounted for ex vivo OCT imaging at the University of Kent. OCT image acquisitions were performed using three fully functional OCT systems (at 850nm, 1050nm and 1300nm), and image characterisation and histological correlation was then performed.

Part of the research team. From left to right: Dr. Jingyin Pang, Dr. Paul J. Tadrous, Prof. Adrian Gh. Podoleanu, Dr. Ramona Cernat, and Dr. Taran Tatla
International links were established with two leading OCT groups (John Hopkins University, USA and the Optical Research Centre Nizhny Novgorod, Russia) who provided technical assistance that resulted in two “forward-looking” small endosopic probe heads, one using 4 piezos and the other using a magnetic principle to scan the optical beam laterally. These were tested for robustness, safety and image resolution/acquisition time ex vivo using an anatomically correct phantom rubber model of an adult head / upper airway to simulate real clinical use. This was a particularly important pre-requisite of the OCT-nasendoscopy procedure before in vivo investigation could commence. These unique international collaborations, involving otolaryngologists and experts in biomedical optics, investigated the utility of OCT imaging in a busy ENT department and obtained pre-clinical data from a novel miniaturized OCT probe utilized for endoscopic imaging of laryngeal mucosa.
Two platforms/instruments for OCT imaging (one dual-channel instrument based on a flexible OCT probe and the other on a hand-held OCT probe) were then transferred from the University of Kent and installed with all necessary components on a trolley at Northwick Park Hospital ENT outpatient department. More details on the two instruments are provided below.
Feasibility studies demonstrated the potential of the dual imaging instrument as a useful tool in the testing and translation of OCT technology from the lab to the clinic. The flexible probe is under investigation as a possible endoscopic screening tool for early laryngeal cancer, while larger size and better quality cross-sectional OCT images produced by the handheld instrument provide a reference base for comparison and continuing research on imaging freshly excised tissue, as well as in vivo interrogation of more superficial skin and mucosal lesions in head and neck patients.
Results of the study were published in Biomedical Optics Express, Vol. 3, Issue 12, pp. 3346-3356 (2012).
Project team
- Prof Adrian Podoleanu Project Technical Lead, Applied Optics Group
- Dr Ramona Cernat Research Associate, Applied Optics Group
- Dr Adrian Bradu Research Associate, Applied Optics Group
- Taran Tatla Project Clinical Lead / Surgeon / Project Manager, Northwick Park Hospital, Department ENT-Head and Neck Surgery
- Paul Tadrous Project Co-Lead / Pathologist, Consultant Histopathologist, Northwick Park Hospital, Department of Cellular Pathology
- Dr. Jingyin Pang, Research Fellow, Northwick Park Hospital, Department ENT-Head and Neck Surgery
Instrument 1. Endoscopic OCT application (via nasopharyngeal tract)

Top: OCT endoscope probe unit terminating in a stainless steel cylinder of 13 mm length and 1.9 mm diameter. Bottom: Flexible OCT endoscope probe and endoscope fiber bundle inserted into a medical grade disposable latex endosheath, with both probe ends sitting flush with the cap.
This instrument was dedicated to in vivo laryngeal investigations, and was based on an endoscope probe head assembled by combining a miniature transversal flying spot OCT scanning probe with a commercial fibre bundle endoscope, thus providing a dual channel nasolaryngeal endoscopy-OCT system. The two probe heads were used to provide simultaneous OCT cross-section images and en face fibre bundle endoscopic images.
This platform involved a slight modification of the current standard nasendoscopy procedure practiced by clinicians in the ENT clinic under topical local anaesthesia. The current procedure uses an endoscope consisting of a multi-fibre bundle producing a white light image on a proximal camera. The bundle is introduced into a disposable, medical grade, endo-sheath and then used to inspect/image the upper aerodigestive tract for pathology. This is done routinely on patients presenting for ENT consultation; a simple procedure completed usually within 1-2 minutes following topical local anaesthesia and requiring no more than verbal consent of the patient. The modification of this procedure involved placement of our own assembled OCT probe to be run in parallel with a 3.7 mm outer diameter commercially available multi-fibre endoscope (typically used for this investigation).
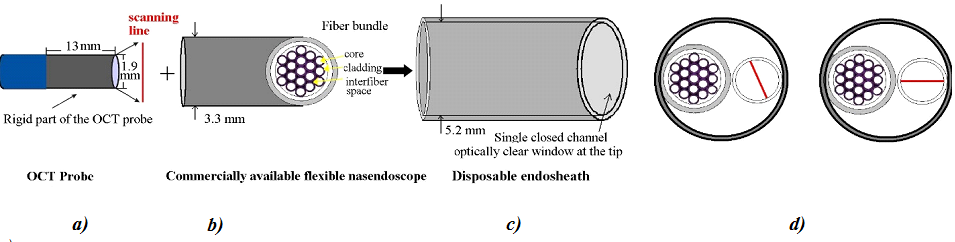
(a) Sketch of the OCT probe (rigid part of length 13 mm, diameter of 1.9 mm). (b) Sketch of a fibre bundle for a standard commercial endoscope (diameter of 3.5 mm). (c) Medical grade disposable latex endosheath with a single closed-channel optically-clear window at the tip (internal diameter of 5.4 mm). (d) Front view of the disposable endosheath with the OCT probe and endoscope fibre bundle placed inside. (e) Correct orientation of the OCT transversal scanning direction.
The two probes sit enclosed within a slightly wider medical-grade disposable endosheath. The rigid part of the OCT probe is 15 mm long and 1.9 mm wide. The combined assembly adds slightly to the width of the inserted nasendoscope but this did not impede the clinician in performing the procedure. Indeed, at present commercially available and used flexible nasendoscopes themselves vary widely in their outer diameters from 2.7 mm to 6 mm or more.
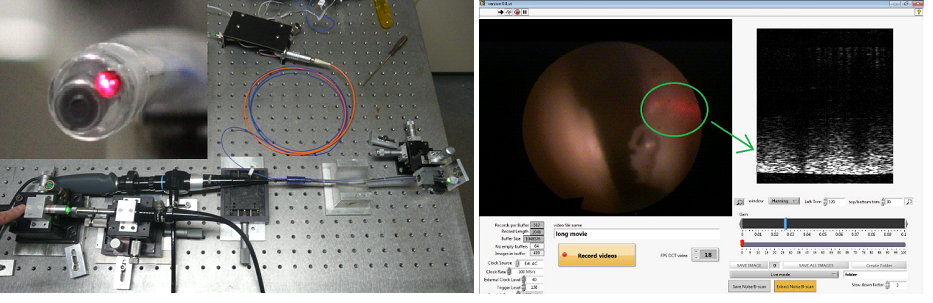
Left: Assembly of the OCT endoscope probe and nasendoscope ready to be tested on the optical bench top. Right: Simultaneous display and recording of “white-light” images in tandem with OCT imaging using the flexible nasendoscope-OCT probe assembly. The red laser guiding beam is used to target the area of interest.
Running the OCT probe together with the camera bundle offered more protection to the patient, as the bundle and the OCT probe were housed inside a single channel, closed-system endosheath. Prior tests on the anatomically correct rubber phantom demonstrated clearly that the integral distal endoscope tip tilting/leverage mechanism is still able to function with the OCT probe sitting adjacent within the endosheath enclosure, providing up to 30 degrees arc of tip deflection. Our tests have shown that this is sufficient to allow the OCT probe to be inserted together with the nasendoscope, housed within the endosheath, the camera providing guidance as the tip is progressed through the nasal cavity and flexed around the contour of the soft palate and nasopharynx to visualise the larynx below. The endosheath is disposed of as clinical waste and a sterile one used for the next patient recruited.
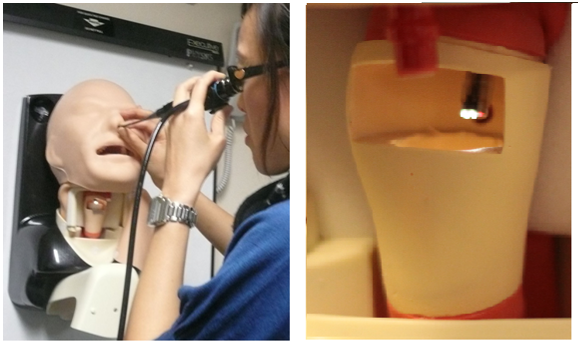
Left: Ex vivo testing of the dual channel OCT probe/endoscope assembly on an anatomically correct adult airway phantom utilized for simulating a standard ENT nasendoscopy office procedure (AirSim Advance Larynx model, Trucorp Ltd for ENT and Aneasthetic training). Right: Laryngeal window opening of the phantom which allows direct external view into the larynx.
As planned in the original study protocol, clinical recruitment was extended to a pilot 40 patient cohort attending NWLH ENT-Head & Neck service, patients who are noted to have suspect larynx lesions on endoscopy. Following informed consent, endoscopic OCT static digital images and digital video was taken before patients went on to have biopsies of the larynx lesion under general anaesthesia. The pathologist compared and correlated the outcomes of OCT optical diagnostic “biopsy” with standard histological biopsy techniques.
Instrument 2. Hand held OCT probe
This instrument was dedicated to either in vivo imaging of accessible surface skin and mucosal lesions of the scalp, face, neck and oral cavity or ex vivo imaging of the same excised tissues, based on a single OCT channel. It was initially tested on phantom models at the University of Kent and then on patients with suspect laryngeal lesions in a busy ENT practice.

Photographs of the hand-held OCT probe platform assembly.
This assembly allows OCT digital still and video image acquisition of more superficial and accessible muco-cutaneous lesions in the oral cavity and skin surface of the head and neck. It is composed of a rigid, hollow plastic tube assembly, measuring 20 cm in length, with an outer diameter of 15 mm and contains a transversal scanner with a lens-associated collimator. These are connected within a hand-held “gun” platform assembly and then via a protected fibre to the OCT engine. Balanced detection is implemented to provide a high sensitivity. After preliminary patient tests, a rigid “spacer” tube was designed for attachment to the distal end of the “gun” assembly, and allowed fixed distance contact with tissue surrounding the lesion in question (to minimise image loss/aberrations resulting from patient movements/operator hand tremor). This rigid “spacer” tube can be dismantled from the hand-held “gun” assembly and sterilised, whereas the proximal length of the tube shaft is protected with a disposable thin latex sheath.
Clinical investigation was focused on a 40 patient cohort with suspected head and neck skin lesions and a 40 patient cohort with suspect oral cavity lesions, all recruited from patients attending NWLH ENT-Head & Neck services. Following informed consent, OCT static digital images and digital video were taken before patients went on to have biopsies of the skin / oral cavity lesion under local or general anaesthesia. The pathologist compared and correlated the outcomes of OCT optical diagnostic “biopsy” with standard histological biopsy technique.
Clincal studies
Two complex platforms/instruments for OCT imaging were transferred from the University of Kent and installed with all necessary components on a trolley to Northwick Park Hospital ENT Outpatient Department
The two OCT platforms were designed to use the same ‘core’ sub-assembly. The OCT platform for the handheld OCT probe used the same optical source, detection unit and visible red-laser guiding beam as for the endoscopic OCT probe platform for use via the nasopharyngeal tract. The main components of these two platforms were assembled in a rigid metallic box with a locking lid and required only input fibre connections to be changed in order to switch from one platform to the other.
Two different digital image acquisition software packages were written in-house to produce, display and record the digital OCT datasets. Photographs of the two OCT platforms designed to use the same ‘core’ sub-assembly installed with all necessary components on a trolley to Northwick Park Hospital ENT Outpatient Department are shown below.
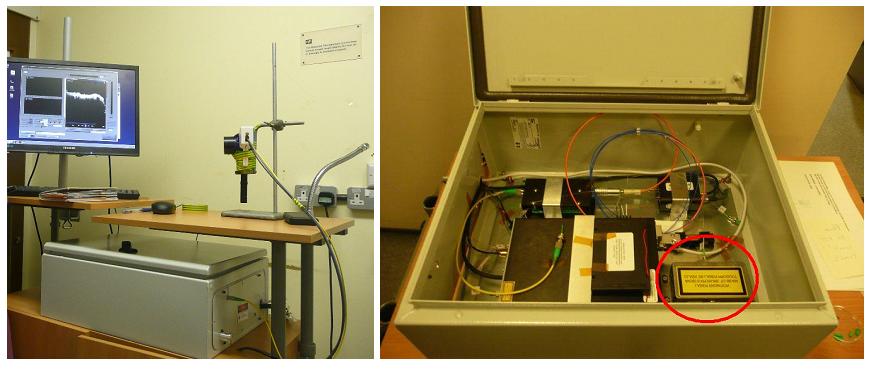
Photographs of the two OCT platforms designed to use the same ‘core’ sub-assembly installed with all necessary components on a trolley to Northwick Park Hospital ENT Outpatient Department.
In-vivo B-scan OCT images of laryngeal lesions were acquired using the endoscopic OCT. The appearance of the left vocal cord lesion using the commercial fibre bundle endoscope, with simultaneous acquisition of B-scan images for the same lesion through the novel endoscopic OCT probe, is shown in (a) and (b) below.
After use of the tool, between each patient, the endosheath was disposed of and a new one used to cover the dual probe head assembly before its use on the next patient. Image (c) below demonstrates the histology for the same laryngeal lesion (invasive squamous cell carcinoma of the left true vocal cord).
Image (d) shows an ex vivo OCT B-scan image of the same left true vocal cord lesion (freshly laser-excised 20 minutes earlier in the operating theatre under general anesthesia), but the image having been taken using the hand-held probe to allow comparison with the in vivo endoscopic OCT B-scan images. Histology confirmed the sample as showing grade 1 to grade 2 invasive squamous cell carcinoma of left glottis (true vocal cord).
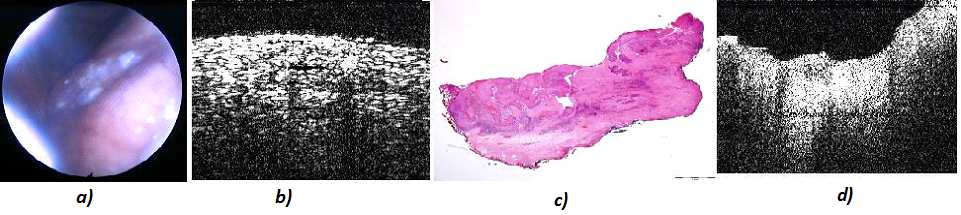
In vivo investigations performed on a patient cohort with suspect laryngeal lesions followed by histology and ex vivo OCT imaging. (a) Fibrescope image. (b) In vivo endoscopic OCT image. (c) Corresponding histology. (d) Corresponding ex vivo OCT image acquired with handheld OCT.
Publications and communications
- Tatla, T., Tadrous, P., Cernat, R., Bradu, A., Dobre, G., Pang, J-Y., Podoleanu, A. Development of Endoscopic Optical Coherence Tomography (OCT) for Laryngeal Cancer Screening – ex vivo data analysis. Abstract published in Australia & New Zealand Journal of Surgery Supplement online at ANZJSurg.com(2011)
- Cernat, R., Zhang,Y.Y., Bradu, A., Tatla, T., Tadrous, P., Li, X.D., Podoleanu, A. Ex vivo OCT Imaging of Larynx Using Forward-viewing Resonant Fiber-Scanning Endoscope Proceedings of SPIE Volume 8213, 82133M, 2012, http://dx.doi.org/10.1117/12.911209
- Tadrous, P., Tatla, T., Cernat, R., Podoleanu, A Histopathological Correlation of Optical Coherence Tomography (OCT) Images of the Human Larynx Ex Vivo Journal of Pathology (Supp) 2012, 226(S1):S.20
- Cernat, A. Jebáčková, A. Bradu , T. Tatla, P. J. Tadrous and A. Gh. Podoleanu, Common path interferometry and light bundles for endoscopy Third Intelligent Imaging Programme, Institution of Engineering and Technology, Savoy Place, 15th June 2011, London, UK (Poster)
- Cernat, T. Tatla, P. J. Tadrous and A. Gh. Podoleanu Ex-vivo data analysis for endoscopic laryngeal cancer screening in a 1300 nm TD-OCT system Optical Coherence Tomography Half Day Meeting, Institute of Physics, 7 September 2011, Portland Place, London, UK (Oral)
- Cernat, T. Tatla, J-Y Pang, P. J. Tadrous, G. Gelikonov, V. Gelikonov, Y. Y. Zhang, A. Bradu, X. D. Li and A. Gh. Podoleanu Ex-vivo Endoscopic Laryngeal Cancer Imaging using two Forward-looking Fiber Optic Scanning Endoscope Probes Abstract submitted for Photonics East Conference, Optics in Health Care and Biomedical Optics V Conference PA103, http://spie.org/x6450.xml
- Tatla, J. Pang, R. Cernat, G. Dobre, P. Tadrous, A. Bradu, G. Gelikonov, V. Gelikonov, and A. Gh. Podoleanu Phantom Testing of a Novel Endoscopic OCT Probe – a Prelude to Clinical in-vivo Laryngeal Use Abstract submitted for Photonics East Conference, Optics in Health Care and Biomedical Optics V Conference PA103, http://spie.org/x6450.xml
- Matela, R. Cernat, J. Wang, X. Zhou, G. Dobre, T. Tatla and A. Gh. Podoleanu OCT Solutions for endoscopy using fibre bundles and micro engines Kent and Medway Health Partnerships Event 28th June 2012 Universities at Medway (Poster)
- Cernat, T. Tatla, J. Pang, P. Tadrous, A. Bradu, G. Gelikonov, V. Gelikonov, and A. Gh. Podoleanu In-vivo Investigations of the Human Larynx using a Flexible Endoscopic OCT Probe Kent and Medway Health Partnerships Event 28th June 2012 Universities at Medway (Poster)
- Cernat, T. S. Tatla, J. Pang, P. J. Tadrous, A. Bradu, G. Dobre, G. Gelikonov, V. Gelikonov, and A. Gh. Podoleanu Dual instrument for in vivo and ex vivo OCT imaging in an ENT department Biomed. Opt. Express 3, 3346-3356, ISSN: 2156-7085, doi:10.1364/BOE.3.003346, https://www.osapublishing.org/boe/abstract.cfm?uri=boe-3-12-3346